
ACHILLES TENDON RUPTURE

Achilles tendon rupture are relative common. Although the Achilles tendon formed by the merging of the tendons of gastrocnemius and soleus, is the thickest and strongest tendon in the human body, it remains susceptible to injury.
During the last two decades, the incidence of spontaneous ruptures has been rising, probably because of the increasing keep-fit culture. Approximately 75% of Achilles tendon ruptures occur during sport activities.
ETIOLOGY
Several aetiological hypothesis have been proposed, including:
• adverse influence of corticosteroids
• fluoroqinolone antibiotics
• exercise – induced hyperthermia
• mechanical abnormalities of the foot
SYMPTOMS
The person who suffers a rupture of the Achilles tendon does not feel pain during a particular time of injury. Just feel a sense of kick the tendon, (someone hit me with stones), and immediately perform a failure of anatomical movements of the foot (a total rupture of tendon)
DIAGNOSIS
The diagnosis of an acute rupture of the Achilles tendon is usually made by a history of a pop or snap in the posterior aspect of the ankle along with onset of mild pain.
Physical examination reveals a swollen, painful ankle with ecchymosis posteriorly. Many patient can still actively plantarflex the ankle against mild resistance because of the pull of the posterior tibial tendon and the long flexor tendon. Inability to rise onto the toes or a heel resistance test, performed by grasping the heel and resisting plantarflexion, showing absence of plantarflexion power are consistent with an Achilles tendon rupture.
The Thompson test has proved to be a reliable test. During this test, the calf muscle is squeezed with the patient prone and the feet extending over the end of the examination table. If the tendon is intact, the foot can plantarflexed. If it is ruptured, the foot cannot move much or at all.
The diagnostic ultrasonography and Magnetic Resonance Imaging confirm the diagnosis.
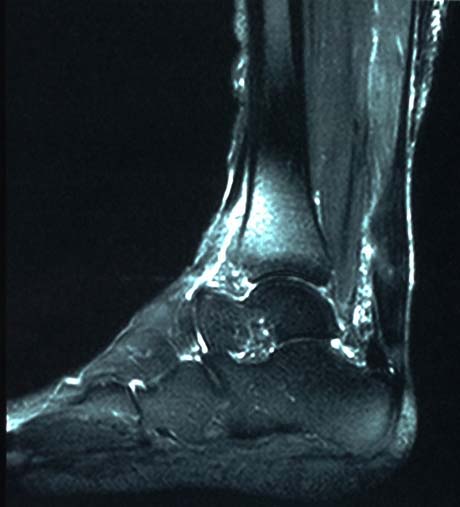
Partial rupture of the Achilles tendon
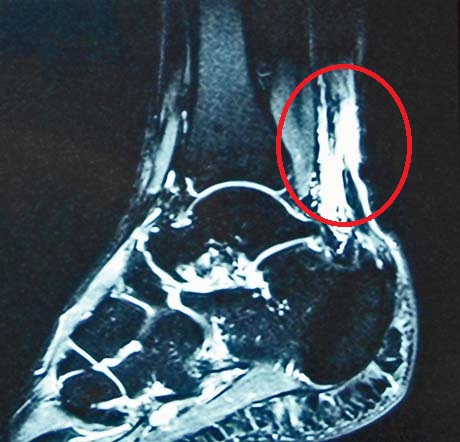
Complete rupture of the Achilles tendon
ACHILLES TENDON RUPTURE. MINIMALLY INVASIVE TREATMENT
ACHILLES TENDON RUPTURE - PERCUTANEOUS TREATMENT
Achilles tendon is the stronger and most historical tendon on the human body. Percutaneous and mini-open surgical repair techniques were developed in order to minimize the potential risks of surgery and to improve functional outcomes.

