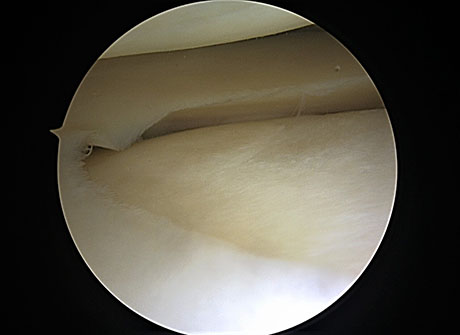
Arthroscopic view: intact medial meniscus in male 42 years old
The rupture of the meniscus of the knee is one of the most common injuries among athletes, but not limited to them. The meniscus is strong, resistant structures that play an important role in the biomechanics of the knee joint. They function as mechanical link allows a better distribution of loads on articular surfaces of the femur and tibia, absorbs vibrations exerted on them, thus contributing to the stability of the knee. About 60% of the joint loads pass through the meniscus.
Horizontal tear of the lateral meniscus (MRI photo)
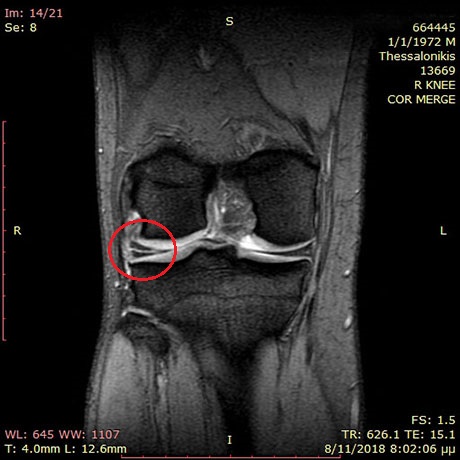
Posterior root rupture of the medial meniscus (red circle)
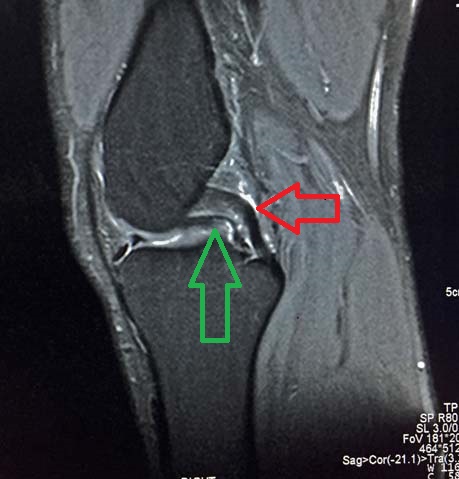
Anterior root meniscal rupture (black circle) Knee MRI: The 'bucket handle medial meniscal tear'. Green arrow shows the rupture of the meniscus. Red arrow shows the intact posterior cruciate ligament.
CAUSE
The meniscus is prone to injury and degenerative processes. The causes can cause rupture of the meniscus is:
• extreme moves such as the knee bends stabilized tread
• too much bending of joints can cause harm by creating large or small lacerations.
• direct trauma (hitting)
SYMPTOMS
The patient may experience:
• mild to severe pain that can readily be resolved by the end of the day in small cases of rupture,
• swelling of the knee which usually occurs after 12-24 hours
• involvement of joints in flexion for an extended break.
• feeling of joint instability
• loss of full range of motion
The injured meniscus is essentially intrarticular foreign body if not treated will cause damage to articular cartilage that is premature osteoarthritis.
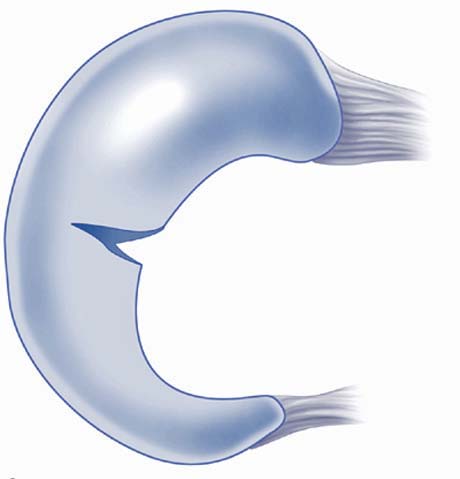
Radial meniscal tear
Parrot beak tear of meniscus
(Operative techniques 'Sport Knee Surgrey" Miller M.)
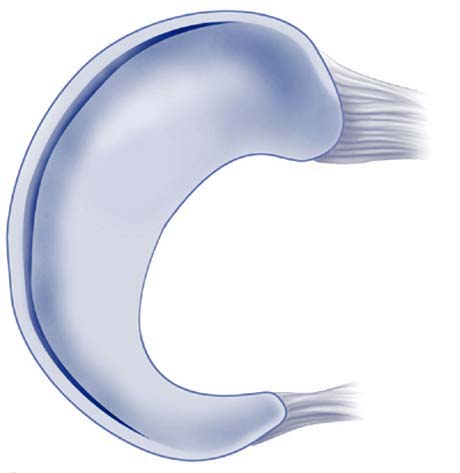
Ventral Longitudinal tear
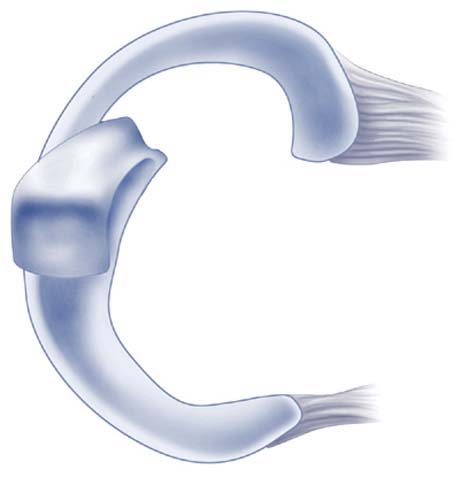
Displaced flap of the meniscus
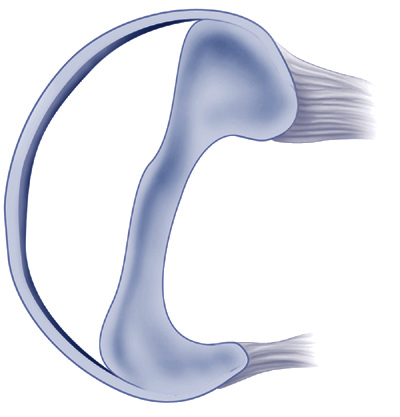
'Bucket handle' meniscal tear that block the knee movement
After the injury must stop any activity to be placed ice around the affected joint.
The visit to the specialist Orthopaedic Surgeon should be done as soon as possible to the clinical examination and the paraclinical testing (radiography, magnetic resonance imaging) to determine the type of injury and design a treatment plan.
Articular cartilage damage to the medial femoral condyle after a neglected medial meniscal tear