
CARTILAGE LESION
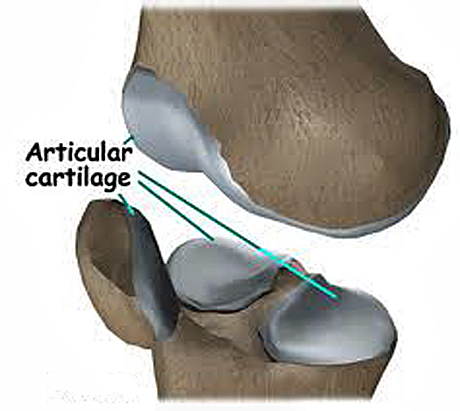
Articular cartilage, also called hyaline cartilage, is the smooth, glistening white tissue that covers the surface of all the diarthrodial joints in the human body. As its name implies, articular cartilage is critical in the movement of one bone against another. Articular cartilage has an incredibly low coefficient of friction which, coupled with its ability to bear very large compressive loads, makes it ideally suited for placement in joints, such as the knee and hip.
Cartilage is composed of specialized cells called chondrocytes that produce a large amount of extracellular matrix composed of Type II collagen (except Fibrocartilage which also contains type I collagen) fibers, abundant ground substance rich in proteoglycan, and elastin fibers. Cartilage is classified in three types, elastic cartilage, hyaline cartilage and fibrocartilage, which differ in the relative amounts of these three main components.
Unlike other connective tissues, cartilage does not contain blood vessels. The chondrocytes are supplied by diffusion, helped by the pumping action generated by compression of the articular cartilage or flexion of the elastic cartilage. Thus, compared to other connective tissues, cartilage grows and repairs more slowly.
ARTICULAR CARTILAGE DAMAGE
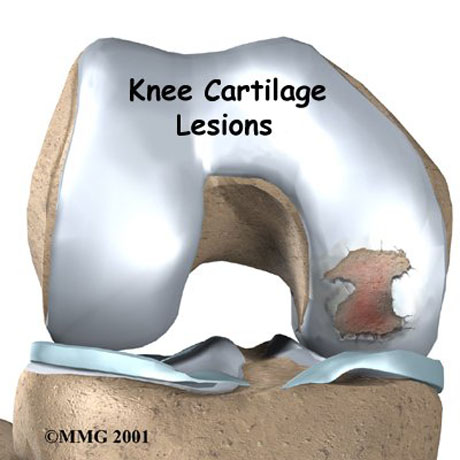
Articular cartilage lesions in people and athletic population commonly occur and result from the significant acute and chronic joint stress associated with high impact activities. These lesions have poor intrinsic healing capacity, and the persistent defect in the joint surfaces cause pain, swelling and mechanical symptoms that result in functional impairment and limitation of athletic participation. If untreated, articular cartilage lesions can lead to chronic joint degeneration and disability. Several techniques for articular cartilage repair have been recently developed with promising results.
SYMPTOMS
• Patients with focal chondral defects generally have symptoms localized to the lesion location.
• Symptoms that worsen with weight-bearing activities likely are produced by damage that resides in the femoral condyle.
• Pain when arising from a sitting position following prolonged knee flexion and with stair climbing suggests a lesion in the patellofemoral joint.
• Patients may complain of activity-related swelling.
An effusion may be palpable, and the affected joint may feel warmer in the presence of an underlying inflammatory process. The ranges of active and passive motion of the knee without effusion are usually within normal limits in the early stages of articular cartilage disease. Localized joint-line pain may be present on palpation, and the McMurray test may elicit some discomfort in the involved compartment. Associated degenerative meniscal tears and articular cartilage disease are commonly associated with older patients. The knee is usually stable to ligament evaluation in most patients, but excluding underlying ligamentous instability is an important part of the examination and future management.
RADIOGRAPHIC IMAGINE
Radiographic imaging of knees with chondral disease should include weight-bearing views for better estimation of mechanical and anatomical axis of lower limb.
Magnetic resonance imaging (MRI) is a useful noninvasive means that may help demonstrate symptomatic articular cartilage lesions. There is often a high correlation with radiographs, but MRI may be particularly helpful when standard radiographs appear normal. Current techniques are more accurate in detecting partial or full-thickness cartilage loss and how large is the damage. These information can define the kind of operative technique which is the right for the patient.

ESSKA Congress, Geneva, Swiss. Poster Presentation.
STEM CELLS AND ARTICULAR CARTILAGE LESIONS
STEM CELLS AND ARTICULAR CARTILAGE DAMAGE

Treatment with autologous adult stem cells represents a promising new perspective on the rapidly evolving field of regenerative medicine and is currently the best alternative method for tissue regeneration. The stem cells are precursors of all cells of the human body and under suitable conditions can be converted into chondrocytes repairing thereby deficits of articular cartilage from the joint injury or due to a osteochondritis dissecans.


