
UNICONDYLAR KNEE ARTHROPLASTY
The painful knee can severely affect the lives of the afflicted, limiting the mobility with adverse effects on general health.
Improved diagnostic methods such as magnetic resonance imaging helped the doctor to better understand the problem, assessing and through these imaging methods, status of articular cartilage, meniscus and ligaments.
The accurate diagnosis has led to more appropriate preoperative planning and the development of new surgical materials and methods or improving existing ones.
One of the biggest developments in recent years in surgery of the knee is the unicompartmental arthroplasty of the joint. This type of resurfacing is less invasive than total knee replacement.
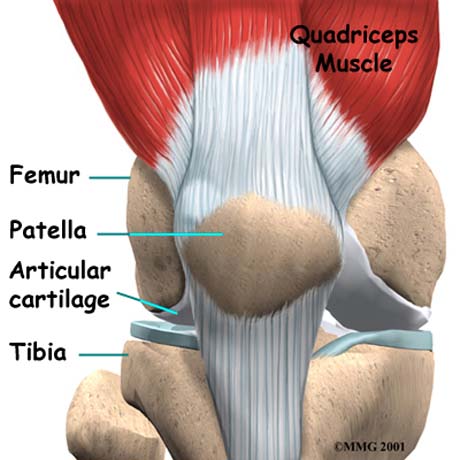
The knee is created by the femur, the tibia and patella. The end surfaces of these bones are covered by articular cartilage that can move one bone relative to another, minimizing friction.
The patella is a bone that is moving in the anterior knee, and over it passes the tendon of the quadriceps muscle and the combination of the patella tendon and creates extensive mechanism athrosis.
The knee is divided on the lateral, the medial and anterior compartment. The lateral compartment consists of the lateral femoral condyle and tibial plateau, the medial compartment of the medial femoral condyle and tibial plateau, and anteriorly consists of the patella and femoral trochlea.
Sometimes osteoarthritis occurs in a single partition of the joint, the medial, the lateral or anterior without serious damage to the other two apartments.
Until recently where they were replacing the whole joint that is known as total knee arthroplasty, sacrificing in this way the healthy femoral condyle, the meniscus and anterior cruciate ligament.
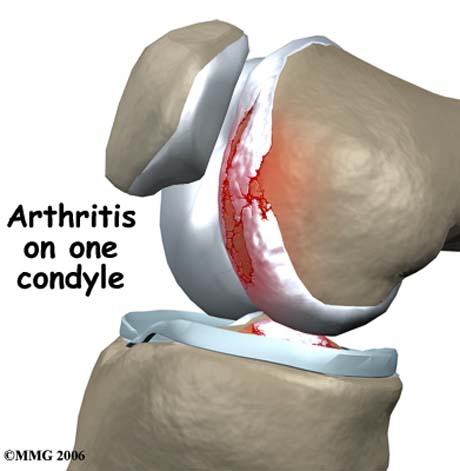
Unicondylar artrhitis
The unicompartmental arthroplasty for the medial or lateral compartment based on the replacement of only one condyle and the corresponding surface of the tibia is affected by osteoarthritis. The main reason for replacing a portion of the joint that suffers is the inhibition of friction between bones no longer covered by cartilage due to wear and cause intense pain.
Implants applied in the affected region provide smooth surfaces that move with ease without causing pain and hence the person undertakes activities that may have been abandoned because of severe symptoms.
This is a significant advantage for younger patients who might need in the future a second surgery when the first will show significant wear rate. Removing less bone during the first surgery, makes easier the implementation of the revision total hip replacement using the knee joint at a future date.
Many orthopedic worldwide use in recent years the unicompartmental artrhoplasty for the treatment of osteoarthritis of the medial or lateral compartment of the knee.
Historically, the first thought is to McKeever in 1950 by inventing the metal intention of a segment of the tibia. Here's Marmor inserting his own unicompartmental implant in the early '70s.
The Marmor's implant was anatomical shape for the thigh section, while the tibial level was composed entirely of polyethylene. Gradually added metal fixture in the polyethylene tibial implant, improving design and construction metals.

OXFORD Unicondylar knee arthroplasty

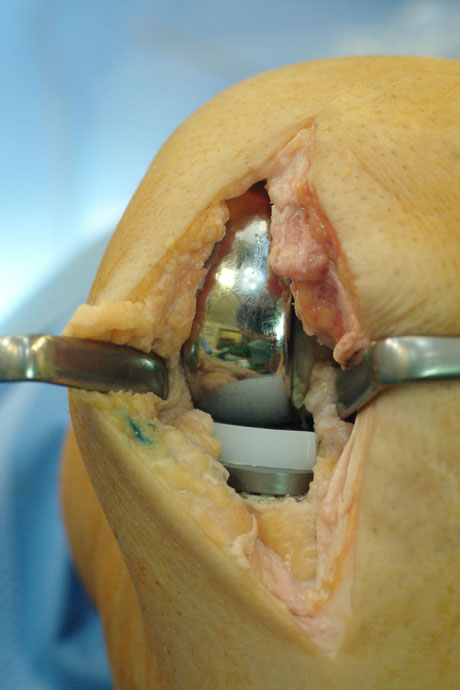
Placement of the femoral and tibial implant
Summarising the unicompartmental arthroplasty has significant advantages over total arthroplasty of the knee joint and these are:
• is a safe surgical procedure with a small wound
• do not need a blood transfusion
• have a reduced risk of infection
• the likelihood of a thromboembolic event is low because they used intramedullary guides
• less time spent in hospital
• lower rate of postoperative pain
THE CONDITIONS FOR APPLYING THE METHOD ARE:
• Preoperative possible correction of valgus or varus knee
• possibility of bending the knee at least 100 º
• extension deficit of the knee area of less than 10 º
• non-inflammatory arthritis - osteoarthritis (not in rheumatoid arthritis)
The permanent deformation of valgus or varus preoperatively creates problems in the implementation of the method. Enhanced strength from the existing types of distortion will be brought to the implant may lead to the premature failure.
The unicompartmental arthroplasty is also contraindicated in people with a weight increase.


X-ray of the knee joint. Unicompartmental knee arthroplasty. The lateral compartment of the joint remain intact.


Direct comparison of total (left side) and unicompartmental knee arthroplasty (right side).
Keeping the anterior and posterior cruciate ligament intact and the other compartment of the same knee and patellofemoral joint, a unicompartmental arthroplasty is that it maintains its normal kinematics of the knee and allows for relatively easy conversion to total hip replacement at a later time.
Also significantly reduced the period of recovery after the joint has greater range of motion in relation to total hip replacement.
The patient after surgery directly weight bearing the operated limb, first by aiding (canes), and faster without it and stay in the hospital 2 days.
The unicompartmental arthroplasty is now an accepted surgical option is included in the quiver of therapeutic treatment of osteoarthritis of the knee in young and elderly patients.

50 plus magazine (Greek edition). Unicondylar knee arthroplasty article

