
CUBITAL TUNNEL SYNDROME
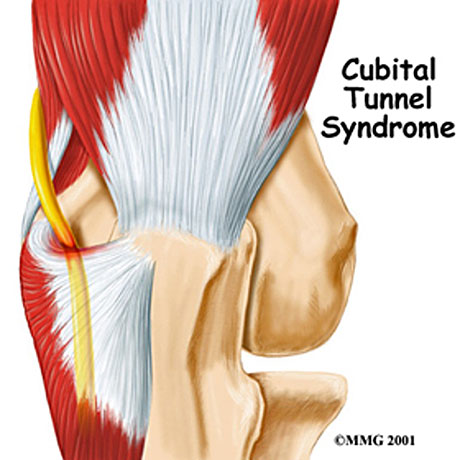
Cubital tunnel syndrome refers to entrapment of the ulnar nerve in its passage around the medial aspect of the elbow. The ulnar nerve normally passes through the anatomic cubital tunnel, which is a fibroosseous ring formed by the medial epicondyle and the proximal part of the ulna.
Beyond the elbow, the nerve travels under muscles on the inside of the arm and into the hand on the side of the palm with the little finger. As the nerve enters the hand, it travels through another tunnel (Guyon's canal).
The nerve functions to give sensation to the little finger and the half of the ring finger that is near the little finger. It also controls most of the little muscles in the hand that help with fine movements, and some of the bigger muscles in the forearm that help to make a strong grip. (bottom right figure)
The syndrome may result from compression, traction, friction, or direct trauma to the ulnar nerve. Compression is thought to be the most frequent cause.
SYMPTOMS
The hallmard complaints of the patients are numbness and tingling in the ring and small fingers and medial forearm pain.
Patients with cubital tunnel syndrome frequently suffer from nocturnal symptoms. In addition, complaints of vague ulnar forearm pain, tenderness on the medial aspect of the elbow and hand clumsiness frequently are reperted. Throwing athletes may suffer from chronic traction injury of the ulnar nerve.


