
MORTON'S NEUROMA
The presence of an Morton’s neuroma between two of the lesser toes must be considered in the evaluation of metatarsalgia. The incidence is highest among middle-aged females, usually presenting unilaterally (85 percent) and occurring in the 3 to 4 interspace (45 percent) more frequently than the 2 to 3 interspace (37 percent). The incidence of simultaneous neuroma in the same foot is rare (less than 4 percent).

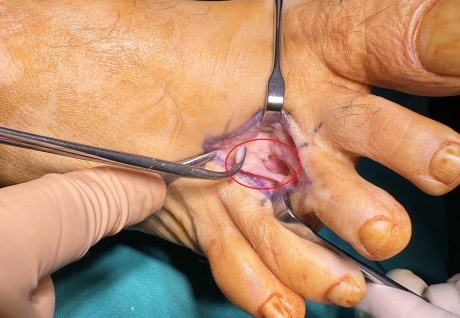
Morton's neuroma
ETIOLOGY
Ill-fitting high heeled shoes provoking increased intermetatarsophalangeal pressures place women at higher risk for the development of a “neuroma” or entrapment of the third branch of the medial plantar nerve (third web space). Chronic irritation of the sole of the foot on business is a serious risk factor for Morton’s neuroma.
SYMPTOMS
The most common presenting symptom is burning plantar foot pain in the involved intermetatarsal forefoot region exacerbated by weight bearing. The pain may extend to the toes.
CLINICAL EXAMINATION
Examination should attempt to differentiate metatarsophalangeal and metatarsal head symptomatology from those symptoms originating from the intermetatarsal spaces just proximal to the metatarsal heads. Gentle compression of the foot across the forefoot, simulating a “tight shoe”, is used to elicit a Mulder’s sign, which tends to reproduce the patients pain dramatically in the involved web space.

Mulder's sign: Indirect pressure of the metatarsal head elicit pain



Direct pressure to the neuroma produced pain
MRI and ultrasonography have been shown to document the location of a neuroma. Weight bearing x-rays are obtained to help exclude other causes of metatarsalgia.

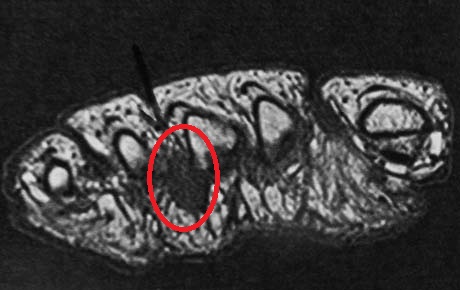

Foot MRI: Morton's Neuroma in the 3rd intermetatarsal space

