Large osteochondral defects of the talar dome, typically involving the talar shoulder (transition of superior dome cartilage to the medial or lateral cartilage), and also often associated with large-volume subchondral cysts.
Cartilage lesions of the talus are focal injuries of the articular cartilage and subjacent subchondral bone may also be damaged.
These osteochondral defect primarily occur as a result of acute and chronic ankle sprains, of repeated microtrauma resulting from chronic instability or fo axial malalignment of the hindfoot.
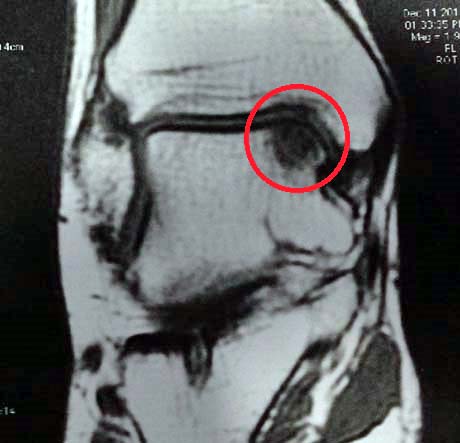
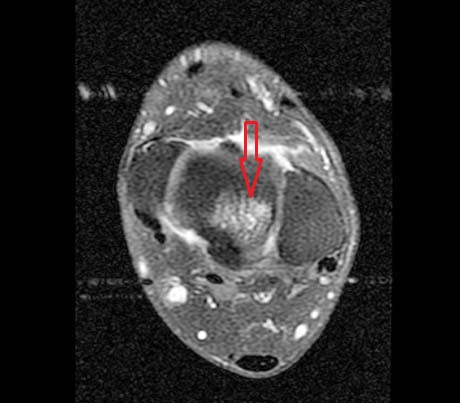
MRI, chondral injury of the medial talus
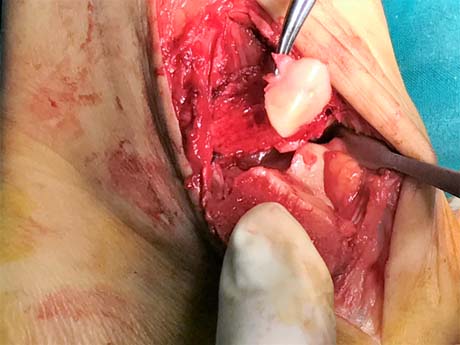
Part of ankle joint cartilage from the upper medial articular surface which is fully detached because the osteochondritis dissecans
The bone defect created in the upper and medial articular surface of the talus after removal of the detached portion
Anatomy of an osteochondral lesion —three zones can be distinguished
• Cartilage: Compared to the knee joint, the ankle cartilage is 1–1.5 mm thinner and less elastic, and has chondrocytes that are more resistant to osteoarthritic damage.
• Subchondral layer: The subchondral bone is essential for the stability of the cartilage. It fixes the cartilage stably to the bone.
• Bone: Bone provides nutrition to the cartilage. Changes of the cancellous structure leading to cysts and sclerosis can be found.
PATHOGENESIS
The pathogenesis for osteochondral lesions of the talus(OLTs) is not fully understood.
Theories include:
• Trauma
• Idiopathic focal avascular necrosis
SYMPTOMS
Persistent load-dependent pain in the ankle joint severely restricts patients in their work and in their leisure activities.
Patients may or may not report a history of trauma
Ankle pain, typically involve the anterior aspect of the ankle, is a common complain.